From History to Today: Smallpox’s Manifestations Return to Modern Day Africa
As explored in this exhibit, the history of epidemics in the United States is one tainted with unethical claims to knowledge and its transference. In the early New England colonies alone, the timeline from the first reported case of smallpox in 1633 to the development of a vaccine by Edward Jenner in 1796 spans almost two centuries. By contrast, from the first reported United States case of the novel COVID-19 virus in January 2020 to the development of the first FDA-approved vaccine in December 2020, we had lived with the pandemic for only eleven months. Though vast amounts of research and medical innovation involving communal knowledge of the ways to effectively eradicate a virus have developed since 1633, most of the negative social implications of epidemics observed in the era of smallpox still hold true.
Excerpts from de La Condamine's book where he has found that smallpox inoculations in West Africa predate European smallpox inoculations.
As seen in the first section of this exhibit From Africa to Europe, the origins of smallpox inoculation occurred not in Europe, but rather in continental Africa, Asia, and the Ottoman Empire. French geographer Charles Marie de La Condamine found that West Africans had been practicing inoculation of smallpox since “temps immémorial” (a time before memory) (de La Condamine in Mitchell, 1773). Here, we must make the distinction between inoculation and vaccination. Inoculation, or variolation, is “the process of transferring smallpox artificially from someone infected with the disease to someone who is not but hopes thereby to contract a mild case and subsequent immunity” and was the technique practiced in Africa (Herbert 539). Vaccination, developed by colonist Edward Jenner in 1796, refers to a similar process, but, in the case of smallpox, immunologically related cowpox is transferred to a patient instead. This technique of vaccination ultimately led to the eradication of and immunity to smallpox. Though we now know that the development of vaccination would likely have been greatly hindered without the stolen knowledge from the African people, the harm against these people of continental Africa was far from over.
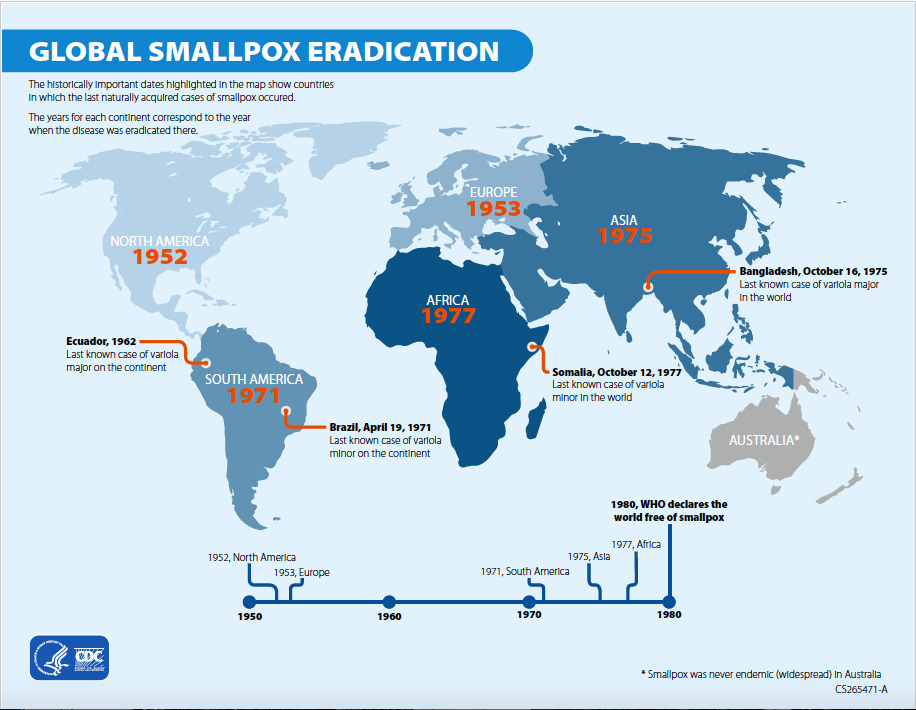
Map from the CDC from 2021 that highlights the fact that the last known cases of smallpox were in continental Africa, and that the epidemic was eradicated there last, in 1977.
Looking into the twentieth century, Americans and Europeans continued to refine and promote vaccination techniques leading to smallpox eradication in these continents in the 1950s. However, the virus remained in Africa until 1977, where the last reported case in Africa was the last case in the world before the WHO declared full eradication in 1980 (History of Smallpox, 2021). See the map of final cases by continent compiled by the CDC to see the exact dates of these final cases, and consider that the epidemic continued to hold prevalence in Africa for two decades after eradication in North America and Europe. The hierarchical structures of past accounts of stolen knowledge manifest themselves again in modern accessibility of medical resources for poorer countries and continents
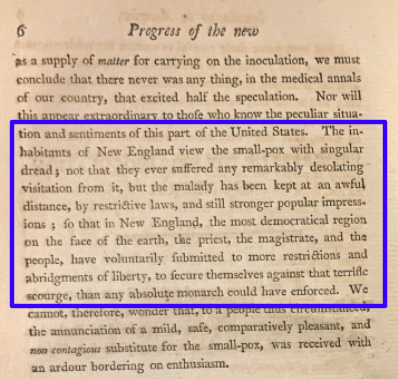
Excerpt from Book of Practical Observations of Variola Vaccinia or Kine Pock by Benjamin Waterhouse, M.D.
Though the smallpox epidemic may seem like a tale of history instead of news, the same injustices of exploitation of knowledge and resources continue to play out in the current COVID-19 pandemic. Despite having neared the one-year anniversary of quarantine in the US, American corporations continue to argue over vaccine access, and some US states are beginning to “reopen” under premises that they are ready to return to their lives again (Goodman and Montgomery, 2021). This sentiment parallels those expressed by white wealthy New Englanders in the early nineteenth century. Dr. Benjamin Waterhouse writes in his novel Practical Observations of the Variola Vaccine that the worst injustice suffered during this epidemic was that New Englanders were removed from their daily lives (Waterhouse, 1802). It seems that these people, too, were ready to return to their normal lives.
Though medical knowledge surrounding pandemics has vastly expanded in the past 350 years, we now find that the social implications remain the same: those who hold privilege in society will take advantage of those without the same privilege, even to the extent in which lives are lost because they are viewed as less important or less valuable to those in power. This sentiment speaks for itself when viewing the map of countries by COVID-19 vaccine access dates. A quick glance at the map reveals that the richest countries in the world, most of which in North America and Europe will have access to the COVID-19 vaccine two whole years before those in poorer countries, most of which are in continental Africa (More Than 85). This cycle of oppression continues to occur right in front of our eyes, as the poorest countries in the world seem to be a mere afterthought in terms of vaccine rollouts. WHO head Dr. Tedros Ghebreyesus spoke out regarding the inequitable rollout of COVID-19 vaccines, saying (Soy, 2021):
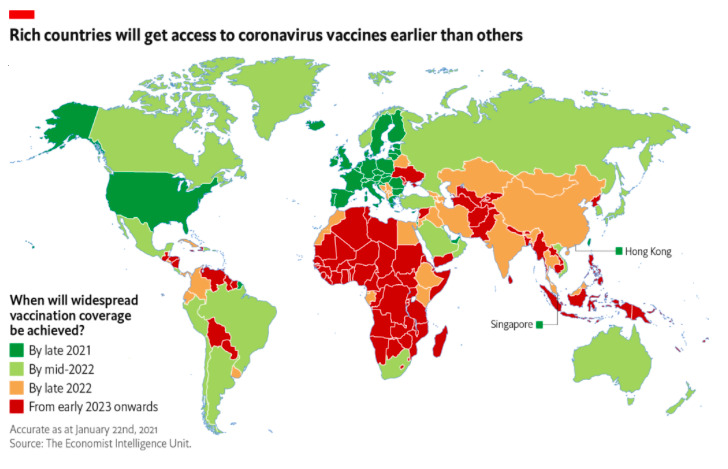
Map compiled by The Economist Intelligence Unit from 02/2021 that shows the delayed vaccine rollout for the poorest countries, most of which are in Africa.
"The world is on the brink of a catastrophic moral failure and the price will be paid with lives and livelihoods in the poorest countries."
– Dr. Tedros Ghebreyesus
Though pandemics tend to highlight the duality of unjust transference of knowledge and power, in reality, these injustices already consume our daily lives. Moving forward as a member of the medical community, an epidemiological historian, or even a concerned member of society, it is of utmost importance to continue educating ourselves in order to work against the monopoly of the medical access assumed by the majority. In what ways do we also play into these hierarchies of knowledge, and how do these questions surrounding medical ethics shape our lives in the twenty-first century? These questions are especially important now, as we begin to consider the ways in which the modern pandemic and those between the era of smallpox and COVID-19 may have played out differently, if credit would have been given where credit was truly due. We now finally begin to consider the ways in which the consequences of stolen knowledge in the seventeenth century are returning back to Africa, in the same unjust way that it was taken from them in the first place.